
Whether steroid causes, a mortality benefit in the severe community-acquired pneumonia (sCAP) remains debatable. Irrespective of the microorganism, lower respiratory tract infection is often associated with a profound host response leading to altered alveolar-capillary membrane permeability, triggering complex systemic and pulmonary inflammatory/immune responses. The host's inability to fully down-regulate systemic inflammation can lead to severe complications due to direct tissue injury and constitute one of the demonstrated causes of increased mortality in sCAP.1
Despite medical breakthroughs, sCAP remains a highly prevalent disease associated with significant morbidity and mortality. The most widely accepted definition for sCAP is the recent severe consensus guideline on managing sCAP in adults.2
Multiple efforts have been made to search for effective modulation of the immune response in CAP, focused almost exclusively on anti-inflammatory therapies. Corticosteroids have been evaluated in numerous studies as a potential treatment option in patients with sCAP without reaching a conclusive recommendation on their use based on poor certainty because of both statistical and clinical heterogeneity, lack of optimal dosing and persistent problems with the imprecision of pooled estimations.3
Recommendations for managing sCAP are usually included as a subsection in general CAP management guidelines; many recommend against the routine use of corticosteroids in patients with CAP, except in cases of refractory septic shock.4,5
However, it has recently published a guideline which provides recommendations on sCAP.2 Based on the results of the meta-analysis performed for the guidelines, the authors recommend using corticosteroids in sCAP patients with septic shock except in severe acute respiratory syndrome (SARS), middle east respiratory syndrome (MERS) and influenza pneumonia. It's, therefore, not surprising that, given the heterogeneity of guidelines, clinical practice regarding corticosteroids for sCAP remains highly variable. In this context, Meduri and colleagues published the ESCAPe RCT,6 which included 584 patients with sCAP (ATS/IDSA criteria) who were within 72−96h of hospital presentation and was a double-blind placebo-controlled study evaluating low-dose methylprednisolone for 21 days (40mg methylprednisolone for seven days, 20mg for seven days, 12mg for seven days) in critically ill patients (Table 1). The primary endpoint was 60 days mortality; no significant differences (16% vs 18%; adjusted OR 0.9, 95% CI 0.57–1.4) were found. However, it is important to stress that the study was stopped early due to low recruitment. Despite a hypothesis that corticosteroids would benefit this population, no effect was found.
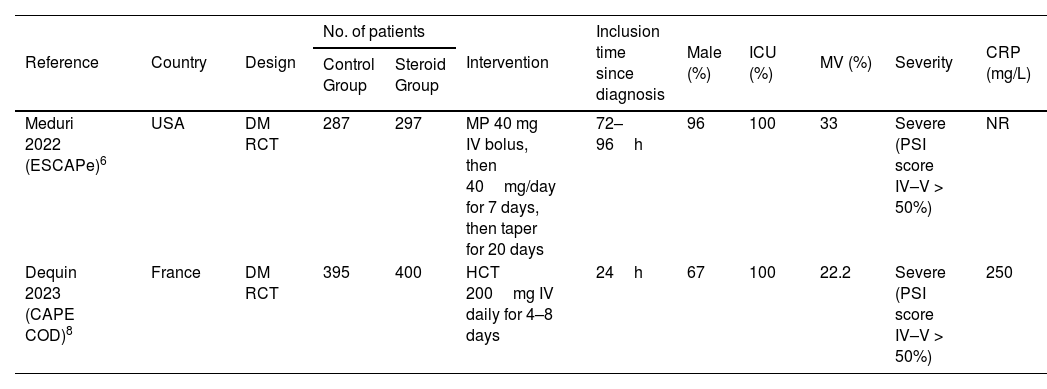
Main RCT Characteristics.
| Reference | Country | Design | No. of patients | Intervention | Inclusion time since diagnosis | Male (%) | ICU (%) | MV (%) | Severity | CRP (mg/L) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control Group | Steroid Group | ||||||||||
| Meduri 2022 (ESCAPe)6 | USA | DM RCT | 287 | 297 | MP 40 mg IV bolus, then 40mg/day for 7 days, then taper for 20 days | 72–96h | 96 | 100 | 33 | Severe (PSI score IV–V > 50%) | NR |
| Dequin 2023 (CAPE COD)8 | France | DM RCT | 395 | 400 | HCT 200mg IV daily for 4–8 days | 24h | 67 | 100 | 22.2 | Severe (PSI score IV–V > 50%) | 250 |
More recently, Saleem et al. published a systematic review and metaanalysis in Chest7 evaluating the effectiveness of corticosteroids for CAP of bacterial origin among adult hospitalized patients, including very recently published data, such as ESCAPe-RCT. All-cause mortality was selected as the primary outcome. Investigators included sixteen trials that involved 3842 patients who were randomized to receive either corticosteroids or placebo. Seven studies included patients with sCAP. The therapy duration and specific corticosteroid administered were different between trials. No association was found between corticosteroid use and mortality, ICU admission and incidence of adverse events, even when the effect of a higher either average daily dose or cumulative dose was considered. However, the authors reported that adjuvant corticosteroids are associated with reducing the need for mechanical ventilation (MV). It is interesting, because it makes us question whether patients with more severe diseases could experience some benefit.
Shortly after that, another multicenter, double-blind, placebo control, CAPE COD trial, with favourable results on the use of corticosteroids in the treatment of severe community-acquired pneumonia, was published by Dequin et al. in the New England Journal of Medicine.8 They included 800 patients with sCAP admitted to the intensive care unit (ICU) who received intravenous hydrocortisone (200mg daily for 4 or 8 days as determined by clinical improvement, tapering for 8–14 days) or a placebo (Table 1). The primary outcome was death at 28 days. There was a significant decrease in mortality (the primary outcome), with 6.2% of the hydrocortisone group and 11.9% of the placebo group dead at 28 days (ARR 5.6%, 95% CI −9.6 to −1.7%, p=0.006). Steroids were most beneficial among patients with a C-reactive protein (CRP) level >15mg/dL (>150mg/L). This is another very high-quality study, with excellent methodology as the ESCAPe trial, but also with the problem of being stopped without hitting the desired sample size, and the mortality was lower than expected, which adds some uncertainty. This trial analyzed a selected group of patients with well-defined pneumonia and clear markers of severity. They excluded septic shock, aspiration pneumonia, influenza, post-obstructive pneumonia, and cystic fibrosis, among a much longer list. This makes us question whether this population represents the patients admitted to our intensive care units.
Pitre and coworkers recently published an updated systematic review and pairwise and dose-response meta-analysis of RCTs,9 examining the role of corticosteroids in patients hospitalized with bacterial CAP, including dose and duration of therapy. Eighteen studies, included ESCAPe and CAPE COD trials and 4661 patients. The authors reported that corticosteroids probably reduce mortality in more sCAP (RR 0.62 [95% CI 0.45–0.85]; moderate certainty) with possibly no effect in less sCAP (RR 1.08 [95% CI 0.83–1.42]; low certainty) and probably reduce risk of requiring invasive MV and ICU admission. This study provides essential contributions evaluated for subgroup effect based on the severity of CAP. This subgroup analysis demonstrates that corticosteroids' impact on mortality is limited to those with severe disease, which aligns with previous studies.
Very recently Wu et al.10 published a systematic review evaluating the efficacy and safety of adjunctive corticosteroids in the treatment of sCAP. A total of seven RCTs including ESCAPe and CAPE COD trials involving 1689 patients, were included. Likewise, in the meta-analysis previously described, corticosteroids' dose, regimen, and treatment duration varied among the include RCTs. The primary outcome was the 30-day all-cause mortality; the authors informed that the overall study group had a lower mortality rate at day 30 than the control group (RR 0.61 95% CI 0.44–0.85; p<0.001). Compared with the control group, the study group had a lower risk of the requirement of MV (RR 0.57; 95% CI 0.45 to 0.73; p<0.001), shorter ICU stay (MD −0.8; 95% CI −1.4 to −0.1; p=0.02), and hospital stay (MD −1.1; 95% CI −2.0 to − 0.1; p=0.04). However, in the subgroup analyses, the differences remained statistically significant only between specific patients subgroups such as ≤ 60 years, with ICU admission, without septic shock on enrollment, use of hydrocortisone and corticosteroid therapy duration of ≤8 days and without corticosteroids tapering.
All the above-mentioned studies6–10 observed no significant differences between the study and control groups in terms of gastrointestinal bleeding, nosocomial infection and acute kidney injury; glucose levels should be closely monitored due to the high risk of hyperglycemia in the study group. However, none studied the long-term effects of corticosteroid use such as myopathy, polyneuropathy and delirium.
With these results, the obvious question is: should we administer corticosteroids to all patients with sCAP?
The most likely answer to this question is no, as there is not enough evidence to change clinical practice as recommended by the guidelines. We should continue administering corticosteroids, preferably hydrocortisone, in those with sCAP with septic shock, as recommended in the recent guidelines. We should extend its use to patients without septic shock but with a high inflammatory profile sCAP determined by a CRP level >15mg/dL (>150mg/L). Such treatment should be administered early, within 24h of diagnosis of sCAP.